Hands-on learning through simulation isa cornerstone in the 21st-century curricula of US healthcareprofessional schools. Standardized patients (individuals specially trained toportray patients), volunteers, and manikins act as patients during simulated patientencounters. Simulations enable students to gain clinical proficiency byapplying classroom and book knowledge to lifelike near-real clinical scenarios.Because these simulations put classroom learning into action, they’reincredibly beneficial to students building clinical knowledge and skills,including interpersonal and communication ability.
Schools like Rosalind FranklinUniversity of Medicine and Science (RFUMS) view simulation as an essential wayfor students to develop communication, psychomotor, and diagnostic-reasoningcompetencies. Rosalind Franklin’s more than 2,100 medical (MD), physicianassistant (PA), physical therapy (PT), nurse anesthesia, podiatry, psychology,and pharmacy students use simulated patient encounters to bridge classroomlearning with clinical practice and gain diagnostic proficiency before theywork with real patients.
But there are tradeoffs: Whiletraditional manikin and standardized-patient-based simulations offer quality student-learningexperiences, they’re often labor intensive for healthcare professional schoolsto coordinate, can be costly to organize, and as a result, happen lessfrequently than needed to help learners progress to mastery. Educators at RFUMSunderstand the value of simulation in health-professions education, but, aswith many other schools, logistical considerations impact how oftenface-to-face simulations can occur.
Beyond the cost and logistics toimplement various types of simulation, there are other limitations to note aswell. Manikin-based simulation puts students in charge of many aspects ofpatient care, but the subtleties of human interaction and bedside manner can bedifficult to replicate on a manikin. Likewise, standardized patients canauthentically portray a case history and many physical exam maneuvers, but areunable to replicate the clinical findings associated with many conditions(abnormal heart and lung sounds, altered vital signs, etc.). These limitationscan pose a threat to engaging learners in a simulation that authenticallyengages the breadth and scope of the complexities in diagnostic reasoning.
In an effort to overcome some of thelimitations of manikin and standardized patient-based simulations, RFUMS hasincluded the use of virtual patients as a complement to more traditional formsof simulation. Through tailored virtual-case studies, RFUMS is helping studentsmaster clinical competencies, diagnostic reasoning, and the clinician-patientencounter through a hybrid approach to simulation-based training.
A hybrid approach to simulation
RFUMS found thatvirtual patients can serve to increase the use of simulation in health-professionscurriculum and provide a simulation-based modality that can compensate forlimitations noted in other forms of simulation. In 2011, RFUMS integrated thei-Human Patients virtual-patient platform into its curricula. Using thisplatform, students interview a virtual patient about symptoms and medicalhistory, perform a physical exam, develop differential diagnoses (hypothesesabout potential diagnoses), order appropriate tests, confirm the diagnosis, anddevelop a treatment plan. Professors see exactly what questions students posed,what exams they performed, what tests they ordered, and review how well the studentperformed in each section. By reviewing the student’s information, professorsprovide feedback and constructive critiques that help students learn from theirsuccesses and mistakes. Students at RFUMS now supplement their traditionallearning with online case studies and virtual simulation in order to sharpentheir diagnostic- and clinical-reasoning competencies while applying theirknowledge to cases that mimic real-life patients.
Diagnostic-reasoning proficiency is acore competency for many students at RFUMS, and virtual patient simulationprovides a method to effectively teach this critical skill set, according toJim Carlson, the dean of the college of health professions and associate vice-presidentfor clinical simulation at RFUMS. Professors conduct virtual-patient casesimulations in the classroom, and in many cases, using a flipped classroommodel, students are assigned a case to complete before a class. The simulationacts as a jumping-off point for classroom discussion and more in-depth analysisand learning.
One method used at RFUMS is a hybridsimulation. For example, students first work through a case on the virtualplatform focused on the cognitive skill of establishing a diagnosis, and thenmay transition to the manikin lab (Figure 1) to test their procedure skills suchas removing fluid from the lungs or inserting a breathing tube as a correctivemeasure for the case presentation. After performing the procedure, studentsreturn to the virtual patient, input their findings, and continue monitoringthe patient.
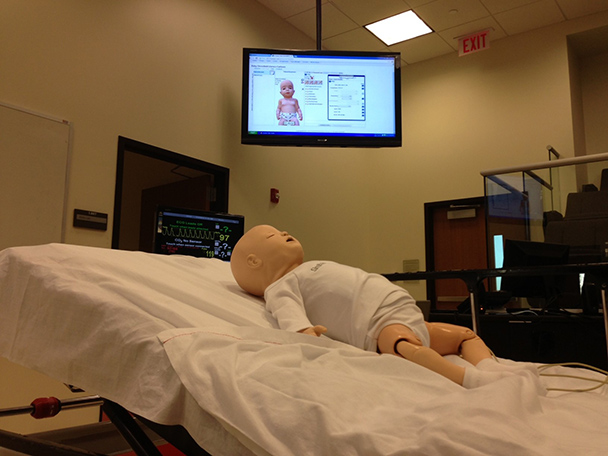
Figure 1: Studentscan test their procedure skills in the manikin lab
“Virtual patient simulation allows us toprovide greater variation and realism in the classroom,” Carlson said. “Now wecan examine the patient in the classroom, and students have to use theirdiagnostic reasoning skills to figure out the problem rather than being toldhow to solve the problem. Virtual-patient simulation has shifted my instructionaway from telling students what they should be considering toward an emphasison honing their own skills and thinking through problems. It adds a layer ofdepth and realism to what we can bring to the classroom, since virtual patientencounters mirror what students will see in the clinical environment.”
Training students in tough-to-teach areas
RFUMS also found thatvirtual patient encounters address many areas of training for which studentexposure is traditionally difficult. Take, for example, geriatric and pediatriccare. Infants, toddlers, and senior citizens are infrequently cast as thestandardized patients that act out ailments. As a result, students rarelyconduct live simulations on real patients in these age groups. Additionally, itis difficult for students to acquire an adequate volume of actual patientexperiences in these vulnerable populations. The use of virtual-patient casesfocused on these hard-to-reach demographics allows RFUMS students theopportunity to acquire experience that is essential to future practice, buthard to achieve through traditional learning formats. (Figure 2)
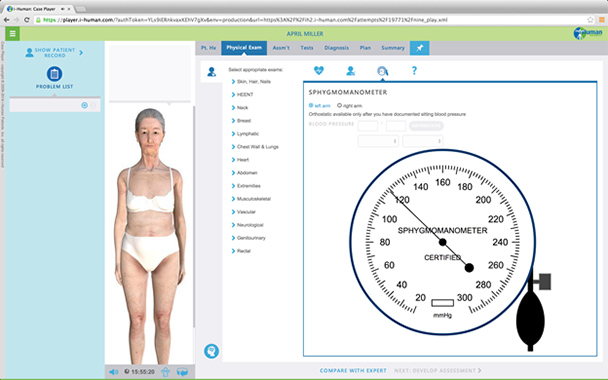
Figure 2:Virtual patient cases (i-Human) allow students the opportunity to acquireessential experience
Obstetrics is anotherarea of medicine that is difficult to teach through actual patient interaction.Clinical rotations are much shorter than nine months, so medical students don’tsee one patient through the entire cycle of a pregnancy. Finding a pregnantwoman willing to be a standardized patient in a live simulation is alsodifficult, so students tend to have very little hands-on experience managing apatient through the duration of her pregnancy.
Virtual patientencounters have helped closed this gap, offering new opportunities to manageobstetrics and pregnancy-related cases, Carlson said. At RFUMS, students interact with virtual avatars who can modelpatients at various points during pregnancy with differing complications. Whenapplicable, students can participate in the delivery of the baby through thebirthing simulator in the manikin lab.
Experience needed—students get it
At RFUMS, students sharpen theirdiagnostic reasoning competencies through scores of virtual cases during theireducation, serving as a complement to face-to-face simulations and actualpatient experiences. Professors have a new way to keep students engaged andactive in their learning, especially in the first two years of MD school orfirst year of PA school where clinical exposure is limited.
Or, as Carlson explained, virtualsimulation gives RFUMS students the ability to test a hypothesis withoutthreatening patient safety. Still, these simulations hold students accountablefor their decisions, and the software can pinpoint mistakes to provide feedbackin meaningful learning, Carlson said.
Because of the availability of thesesimulations—accessible anytime and anywhere there’s an Internet connection—studentsnow have the ability to constantly test and refine their diagnosticcompetencies. In turn, they grow more adept at diagnosis and management bothbefore working with actual patients and as they continue to develop theclinical ability.
Many graduates of the school’s MD and PA programs have citedtheir virtual simulation experiences at RFUMS as beneficial to their earlyinteractions with patients. According to Carlson, this training has helpedstudents develop their competencies in pre-clinical training, and refine theirdiagnostic proficiencies and clinical reasoning before participating in thecare of actual patients.
The future of medicine and simulation
Acquiring clinical competency is complexand time intensive. Manikin and standardized patient simulations haveestablished themselves as a core part of healthcare education. But these simulationscan be time consuming and difficult to coordinate, and they don’t always coverthe full gamut of patient-care experiences needed to provide doctors and PAswith a well-rounded education.
Virtual patient simulations, now being used in UShealthcare professional schools like RFUMS, can better shape the diagnostic andcritical thinking skills of students than other forms of learning. Thesesimulations can be used in classrooms to provide another layer of learning asindependent homework, as a standalone group-learning tool, or as a complementto other forms of simulation. Now and in the future, students will gainvaluable experience by working through virtual cases and simulations, as theydevelop diagnostic reasoning and hone clinical-care skills to ensure the bestpatient outcomes.